Summary
You need to handle medication reconciliation during surgery scheduling and also during post discharge.
Why is it important? Research data shows that:
- Medication errors leading to adverse drug events. Adverse drug events (ADE) account for 4.7% of hospital admissions (USA)
- An estimated $3.8 MM is spent per year per hospital on adverse drug related events.
- Further research data shows that $1 MM of that $3.8 MM spend is preventable
- 60% of all medication errors in the hospital occur during admission, intra-hospital transfer or discharge. This can apply to admission and discharge from ambulatory surgery centers as well.
- Finally, 53.6% of pts have at least 1 unintended medication discrepancy
One of the top ways to avoid medication related errors and expenditures is to perform medication reconciliation at each point of transition of care.
Medication reconciliation steps
Medication reconciliation is simple if you follow this logic
- What medications is the patient taking now?
- What medications do you want to prescribe?
- What’s the delta between these two?
- Would there be any adverse effects in the reconciled list of medications you want to prescribe?
- Prescribe the reconciled medications list.
That’s it. If you use a surgery scheduling software, you would note these as follows

Surgery scheduling -Medication reconciliation
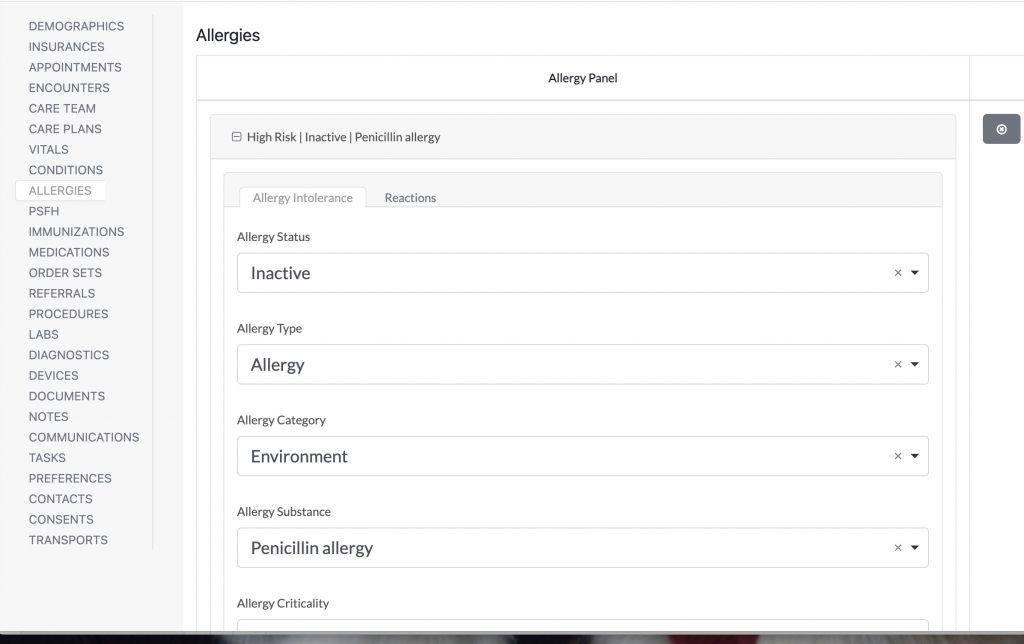
During surgery scheduling, you will invariably have to perform medication reconciliation. Allergies reconciliation is a sub part of medication reconciliation. When you are documenting a patient’s allergies make sure that you document the type of allergic reaction and the severity of that allergic reaction as well. Severe anaphylactic reactions are the not the only ones to be wary of.
One way of handling this could be to ask the patient to bring in all the medications they are taking, during their next encounter. This allows the provider to sort out the drugs and to perform reconciliation. However, that only covers the drug related allergies and leaves out others.
What to include in medication reconciliation
For clinical best practices and as per CMS, the following need to be part of your medication reconciliation.
The most accurate list of
- All medications that the patient is taking
- Include full medication name
- Full medication dosage
- Frequency the medication is being taken
- Medication route (how the medication is being taken/administered)
If you use our surgery scheduling software, you would enter those details like so:

Standard medication reconciliation processes
You can standardize your medication reconciliation processes and ensure that the same format of questions are asked at each patient encounter.
Or if you use a medical CRM, the system can call the patient on a regular basis to gather all allergies related information.
Such medical CRM systems can also perform medication reconciliation on your behalf.
Medication reconciliation – Penicillin allergies
Keep in mind that Up to 98% of penicillin-allergy labels are incorrect when actual testing was done. In other words, your surgery patient might tell you that they are not allergic to penicillin but unless they can substantiate the claim with a relatively recent test result, make sure to order this test.
As you’re scheduling a surgery, make sure that you ask the patient about their drug related allergies, paying special attention to penicillin related allergies . Many times patients are not actually sure that they might have penicillin allergy because they’ve never been tested before nor have been in a situation where such a test was warranted.
Dig deeper when a patient responds negatively to “are you allergic to penicillin “.
According to research, penicillin remains a leading cause of drug-induced hypersensitivity and anaphylaxis. Amongst fatal drug-induced anaphylaxis, penicillin was the most commonly identified culprit drug in a recent US study.
While penicillin related allergy has reduced from 15% to approximately 3% over the years, the evidence of harm still looms large.
Penicillin allergy outcomes include infection and antimicrobial resistance, hospital readmission rates, length of hospital stay (increased use of critical care beds). Postoperative surgical site infections (SSIs) are major contributors to patient morbidity and mortality, and therefore, costs.
You can collect allergy information in our surgery scheduling software like show below:
Preoperative penicillin allergy questionnaire
Keep it simple
- Does the patient know if they’re allergic to penicillin?
- How does the patient know their penicillin allergy status?
- Has the patient ever had a penicillin allergy skin test?
- When did the reaction occur?
- Penicillin to which patient reacted?
- Unknown
- Penicillin
- Amoxicillin
- Amoxicillin-clavulanate
- Ampicillin
- Ticarcillin
- Piperacillin
- Cloxacillin
- What was the reaction from this allergy?
- Hives – red, raised, itchy bumps
- Shortness of breath/wheezing
- Swelling of the eyes, face, lips, tongue
- Hypotension
- Nausea, vomiting, diarrhea, cramping
- Severe cutaneous reaction
- Other type of rash
- How soon after taking the medication did the reaction occur?
- Has the patient received penicillin since the reaction?
Gather as much information on these reactions as possible (e.g. see how it is done with our surgery software)

Medication reconciliation – Latex allergies
Many surgical supplies, devices, gloves, syringes, catheters contain natural rubber latex (NRL). Over the years, NRL (latex) has become a major problem for patients (surgical or non surgical) due to allergies to latex (known or unknown to the individual). These allergic reactions can be minor (redness, itchiness) or can be as severe as asthma or anaphylaxis.
Latex allergy has no cure, but can certainly be managed.
If you have a surgical patient labeled as latex allergic, it’s best to schedule their surgery as early during the week and day as possible. This minimizes your risks.
An OR team typically has to assemble a latex-free supply cart for such patients. Hence, identifying surgical patients with allergies allows for proper preparation.
Preoperative latex allergy questionnaire
You need to know which patients are more prone to latex allergies. These include but are not limited to
- Healthcare workers (they frequently wear latex gloves)
- Individuals that have undergone multiple surgeries
- Non healthcare workers that have frequent contact with latex gloves owing to their profession (eg cleaning personnel, individuals working in plants, hairdressers etc)
- Children with birth defects, born prematurely
- With food allergies (avocado, banana, chestnut – high risk. Apple, carrot, celery, kiwi, melon, papaya, potato, tomato – intermediate risk. Low risk – apricot, cherry, fig, grape, hazelnut, mango, nectarine, passion fruit, peach, peanut, pear, pineapple, plum, rye, soybean, strawberry, walnut, wheat).
- Patients that have or had asthma, dermatitis or eczema
Ask the patient a few simple questions. If there’s any doubt, create a specialist order (allergist).
- Has a physician ever told you that you had a latex allergy?
- Are you aware of being allergic to foods like avocado, banana, chestnut, apple, carrot, celery, kiwi, melon, papaya, potato, tomato?
- Have you ever had allergies, asthma, hay fever, eczema, or problems with rashes?
- Have you ever had any allergy symptoms after being in contact with a diaphragm, condom, balloon, rubber gloves, dental exam etc?
- Have you ever had respiratory distress, rapid heart rate or swelling?
Your job is to make sure that your patient and your healthcare setting is de-risked. Don’t make clinical decisions yourself- refer that patient out to an allergy specialist.
Allergist referral order in surgical scheduling
If your patient cannot substantiate not being allergic to penicillin, order an allergist referral while scheduling their surgery.
Order a skin prick test (SPT) / intradermal test (IDT). The skin test pre-screens patients for a drug provocation test (DPT). Patients who do not react to SPT or IDT are unlikely to react severely to the DPT.
It’s better to be safe than sorry.
Transition of care medication reconciliation
CMS requires you to perform medication reconciliation post-discharge. There are quality measures attached to this. CMS wants 100% of patients to receive a medication reconciliation within 72 hours of discharge.
Transition of care, inevitably, requires a high level of care coordination. As per CMS, care coordination must include medication reconciliation post-discharge.
This affects your own HEDIS scores as well.
Handling allergies during TOC
Make sure to share all allergy information with both the primary care provider and the pharmacy of your patient’s care team. This enables higher levels of transition of care – inevitably, better continuity of care as well.
Urgent surgeries – handling allergies
If surgery cannot wait, make sure that the patient gets their testing done before the surgery, at the surgical healthcare setting. If by any chance you have access to the patient’s prior records, make sure that your anesthesiologist gets access to that. They might want to avoid all drugs used in the previous surgery. Otherwise, anaesthesia should proceed using the lowest risk drugs (I.e no neuromuscular blocking agents NMBAs , no chlorhexidine, no latex).